Recognition of Medical Optometry
Formed in 2009, the American Board of Certification in Medical Optometry is now recognized by credentialing committees at over 100 Joint Commission accredited medical facilities across the nation that have appointed ABCMO certified optometrists as specialists in medical optometry rather than general practice.+ Specialists hold Level 2 credentials after completing an accredited specialty residency, passing a national specialty examination and certification by a recognized specialty board.
This acceptance of ABCMO certification established medical optometry as a recognized specialty and resulted from its adoption of specialty requirements analogous with those required of specialists in medicine, osteopathy, dentistry and podiatry.
Facilities Recognizing ABCMO Certification
Accredited medical facilities recognizing ABCMO specialty certification include:
- Federal hospitals: Department of Veteran’s Affairs medical centers and clinics, Army-Navy-Air Force hospitals and clinics, Walter Reed Medical Center and Indian Health Service of the US Public Health Administration. (79 facilities to date)
- State Licensed Hospitals: Notably the Mayo Clinic and University Hospitals. (24)
- Credentialing documenters: CHG Healthcare, Air Force Centralized Credentials Verification Office, CVS, Valforce, VeriPoint, Merrit-Hawkins, Aperture. (7)
- Private eye practices. (26)
- Academic teaching facilities. (7)
ABCMO has now certified 418 optometrists to date, of which over half are members of the medical staff at accredited federal hospitals and clinics.
The typical ABCMO certified optometrist is an AOA member, Fellow or Section Diplomate of the American Academy of Optometry, faculty at an affiliated school of optometry and medical staff member at a Joint Commission accredited medical facility (federal and state).
Joint Commission accredited facilities conduct mandatory re-credentialing reviews of their medical staff and now require verification of ABCMO certification during credentialing reviews.+
With 24% of optometry school graduates completing specialty residencies other nascent specialties may soon seek recognition. The American Board of Optometry Specialties, sponsored by ABCMO, is prepared to assist in their development.
Note: While medical optometry residencies began at Veterans Affairs hospitals, optometrists completing accredited residency training in medical optometry at schools and non-VA facilities may apply for ABCMO certification. About 35% of ABCMO certified optometrists did not train, or practice at a federal medical facility. This percentage will continue to increase with the growth of non-VA medical optometry residencies.
VA Optometry Residencies
In 1946 the VA was first directed by Congress to establish medical residencies but VA optometry residencies for optometrists did not begin until 1975.
Congress realized in 1945 VA hospitals were ill prepared to care for the large numbers of WWII veterans and authorized building new VA hospitals affiliated with medical-dental-nursing schools, higher pay schedules and VA student intern and residency training programs for physicians, dentists and nurses. Today the VA is the largest component for training interns and residents in the country via its teaching affiliations.*
Unfortunately the 1946 VA modernization did not include optometry staff or affiliations with schools of optometry that continued to lack access to medical facilities, even at universities with medical and optometry schools and a nearby VA hospital.
To be fair, optometry’s isolation from hospital-based training was due to both its fear of being absorbed by medicine and a now expired AMA decree barring physicians from taking part in optometry training. In 1970 the VA still employed but 9 elderly Civil Service optometrists and had no optometry school affiliations but did have backlogs of veterans seeking eye care. Studies by schools of optometry, the American Optometric Association and the U.S. General Accounting Office documented VA lacked optometry staff, equipment, teaching affiliations and adequate salaries; the same conditions that had existed in 1945 for VA medical, dental and nursing care before VA modernization.
As in 1946, Congress responded to those findings by enacting legislation in 1976 that authorized a VA Optometry Service, transferred VA optometrists from Civil Service to the VA Medical-Dental salary scales and mandated optometry teaching affiliations; actions mirroring those of 1946 for VA medical, dental and nursing programs. As a result VA optometry care rapidly increased in quality and availability.
In 1975 the Kansas City VA hospital affiliated with the U. of California at Berkeley School of Optometry to create the first hospital optometry residency in the nation, training optometrists for hospital-based practice, a new area of optometry training.
That residency proved so effective other VAs developed optometry residencies and optometry student intern rotation programs expanded with them. (The first student rotations began in 1973 at the Birmingham VA hospital in affiliation with the University of Alabama, at Birmingham, School of Optometry.)
Today 70% of optometry students complete at least one VA rotation before graduation and the VA now has over 725 full-time optometrists on its medical staffs; operates 86 optometry residency programs training 215 optometry residents per year and VA optometry clinics have over 1.4 million unique patients enrolled.
NAVAO Calls for Specialty Exam
At its annual meeting in 1998 the National Association of VA Optometrists (NAVAO) decided a standardized examination to test the competency of those completing VA optometry medical optometry residencies was a high priority.
NAVAO believed this specialty examination would address concerns of the VA Office of Academic Affiliations that while VA residencies in medical optometry were popular and accredited, there was no quantitative measure to assess the competence of those completing them. And, after extensive meetings between NAVAO and the National Board of Examiners in Optometry (the profession’s independent testing body utilized by optometry schools and state licensing boards), a joint working committee developed the written specialty examination, “Advanced Competence in Medical Optometry” (ACMO), first administered in 2005 and thereafter annually.
The ACMO examination was the second step in developing medical optometry as a recognized specialty, and is a metric by which the VA, optometry schools, and ABCMO can assess medical optometry residency programs at VA and non-VA facilities.
While the majority of VA residency programs emphasize medical optometry, there are others that emphasize “low vision” and “vision rehabilitation” that can be expected to develop similar examinations and certifying boards in the future.
Establishing ABCMO
ABCMO organized in 2009 to certify optometrists who completed an accredited postgraduate medical optometry residency at an accredited medical facility, passed the ACMO examination and met other professional requirements. Establishing ABCMO allowed medical optometry to meet all three requirements of a recognized specialty—Specialty Residency, Specialty Examination, Specialty Board certification.
This process took 34 years and required close cooperation between the VA, the nation’s schools of optometry and the profession’s residency accrediting body.
While a slow process, thirty-four years was also typically the time required to establish specialties in medicine and dentistry.
In return for its support the VA has benefited from team delivery of eye care, better relations between medicine and optometry, reduced waiting times and creation of a national pool of hospital-trained optometrists from which it can recruit. A higher percentage of VA medical optometry residents practice in the VA than any other specialty. For example, the current national Director of the VA Optometry Service completed a VA residency, served as a VA staff optometrist and a VA Optometry Section Chief prior to appointment in Central Office.
Nature of Specialty Training and Certification
Specialty boards began to appear first in medicine as it broadened in scope to the extent a physician with an internship after graduation, could not be competent in all areas. The first specialty organized in 1930. With time, specialties formed coordinating bodies to develop uniform standards for residency training, specialty examinations and certification boards. Early boards had “grandfather clauses” to allow older practitioners to be certified without serving a residency; these usually expired within 5-years of the board’s creation. Certifications were life-long but today many certifications expire after 10 years with re-certification required via programs of Maintenance of Certification.
The system for training and certifying medical specialists developed at clinical facilities and arose sui generis, rather than by fiat from medical schools or state licensing bodies (the latter play no role in certifying specialists). The current coordinating body for allopathic physician specialists is the American Board of Medical Specialties (ABMS).
Credentialing of Medicare Physicians
Five prescribing health professions [allopathic-osteopathic Medical Doctors, Dentists, Optometrists and Podiatrists], are classified by the Centers for Medicare and Medicaid as “Medicare Physicians”.
This is the peer group into which optometry credentialing must be compatible with as federal medical agencies use one, standardized qualification credentialing form for them.
In this credentialing system Medicare Physicians holding a state license are credentialed as general practitioners of their profession [Level 1 credentials]; Specialists, by completing a postgraduate specialty residency, passing a specialty examination and being certified by a specialty board hold Level 2 credentials. Sub-specialists, have fellowship training within a sub-specialty recognized by their specialty board and hold Level 3 credentials.
Most (90%) allopathic and osteopathic physicians hold specialty certifications but considerably fewer of the other three Medicare Physician are specialists because their state licenses already limit their scope of practice. Optometry has one specialty board.
Requirements for Specialty Recognition
Medical and osteopathic physicians, dentists, podiatrists and optometrists have separate, independent governing bodies for their specialties but share in common these key requirements for recognizing specialists:
- Hold a clinical doctoral-degree from an accredited medical, osteopathic, dental, or podiatry school.
- Complete an accredited, postgraduate residency in a defined specialty.
- Hold a letter of endorsement from the Chief of their residency program.
- Acquire a state license to practice their profession while in residency.
- Following residency, pass the standardized national examination testing competence in their specialty required by their specialty certification board.
- Meet additional requirements for certification by their specialty board such as nature/site of residency training, numbers of patients seen, recommendations of former residency supervisors and evidence of high moral character.
At this time there are over 30 recognized specialty certifying boards for allopathic physicians, 18 for osteopathic physicians, 9 for dentistry, 1 for optometry and 6 for podiatry.
Sub-specialists are credentialed by the specialty board of which they are a certified specialist after serving a fellowship in the sub-specialty.
Optometry Specialties Slow to Develop
Optometry educators have identified areas suitable for specialization but only medical optometry has accredited residency programs, a standardized specialty examination (ACMO) and a specialty board recognized at Joint Commission accredited hospitals. Approximately 8% of optometrists practice within those accredited medical facilities.
While optometry’s legal and educational scope of practice have continued to widen, its national organization has seemed reluctant to endorse specialization although over 20% of graduates pursue specialty residency training. But specialization among the other licensed health professions has taken place with Pharmacy one example.#
In 1986 a committee of the American Optometric Association proposed guidelines by which a specialty could be recognized by nonprofit specialty boards external to the AOA. But its House of Delegates voted against approving this and the AOA still has no policy on optometry specialties. ABCMO choose to align with those AOA guidelines and those of recognized specialty boards in medicine, osteopathy, dentistry and podiatry.
Earlier, the American Academy of Optometry in 1984 had examined the issue of specialization and certification and its Executive Committee concluded “being a fellow in the Academy” or a “section diplomate” did not constitute certification of clinical competence as they were “knowledge based” rather than “competency” based.
ABCMO therefore has had to emerge independently (like early medical specialty boards) and establish recognition by its acceptance at Joint Commission accredited health facilities as a Level 2 credential within the “Medicare Physician” credentialing system.
In summary, the three levels of staff appointments made at Joint Commission accredited health facilities for “Medicare Physicians” are:
- Level 1: Degree and license to practice.
- Level 2: Level 1 + specialty residency + board certification.
- Level 3: Levels 1 and 2 + fellowship training within sub-specialty.
+ The Joint Commission (formerly Joint Commission on the Accreditation of Health Care Organizations) is the recognized gold standard of health care facility accreditation.
* The Dept. of Veterans Affairs and Department of Defense (DOD) are separate Federal Agencies. VA cares for those discharged from active duty while DOD health systems care for active duty personnel and dependents. Retired military personnel are eligible for care from the VA or DOD.
# Though not considered “Medicare Physicians”, the Board of Pharmacy Specialties was organized in 1976 as an independent agency of the American Pharmacists Association and it recognizes five areas of specialty pharmacy practice: Nuclear Pharmacy, Nutrition Support Pharmacy, Oncology Pharmacotherapy and Psychiatric Pharmacy.
Appendix
Background
The factors and legal background leading to the formation of ABCMO and its credentialing standards are detailed here:
These links provide perspective and supplemental material explaining the ABCMO mission, why VA pioneered medical optometry residencies and the agreement of ABCMO criteria with standards and requirements of specialty certifications in medicine, dentistry and podiatry.
The Role of State Licensing
The majority of optometrists are in private practice for which the legal requirements are an O.D. degree from an accredited school or college of optometry and valid, current state license to practice optometry. The states, not the Federal Government issue licenses to physicians, dentists, optometrists and podiatrists as well as to non-medical practitioners (insurance agents, realtors, barbers, brokers, opticians, beauticians, etc.) State licensing boards do not regulate specialists other than requiring them to hold a state license.
Advent of Medical Specialists
Prior to WWI the majority of physicians were in private practice and had completed a one-year internship. Their training was geared to the solo practice of general medicine. With the spread of hospitals and beginning development of medical specialties, some young physicians sought specialized training by spending time with a hospital-based mentor.
One of those physicians was W.J. Mayo of Rochester, Minnesota who set aside time each year to study with an expert in a specific area. In 1894 he visited the new school of medicine at Johns Hopkins University, in Baltimore, where he met Dr. William Osler. Johns Hopkins was held as an example of how modern medical schools should be organized and had adopted the German style of medical education where permanent “chiefs” ran specialty clinics at which recent medical school graduates “resided” to study a specialty.
Dr. Mayo, impressed by this system, joined others in endorsing the Johns Hopkins model and adopted it for what is now the respected Mayo Clinic System. From this developed the “residency” training model. The Mayo Clinical System was among the first to accept ABCMO certification.
These residency “rules” were first established at Johns Hopkins:
- Specialty training is at the postgraduate level.
- This training is conducted within an accredited hospital under a specialty “chief” who is usually a faculty member at an affiliated medical school.
- Residency training centers on patients suffering from conditions upon which the “chief” is an acknowledged expert.
- The residency training center has sufficient patient flow to practice its specialty full time.
- Residents are given greater responsibility for patients in graduated steps.
- Residents are, mentored, monitored and “tested” during training.
- When the “chief” believes a resident is qualified to practice the specialty the resident is given a “voucher of competence”.
The “voucher of specialist competence” was a letter from the residency “chief” attesting to a resident’s competence which evolved into a specialty certification process.
The Move to Board Certification of Specialists
Medical doctors are free, once granted their medical degree and license (which requires serving an internship of 1-2 years after graduation) to establish the type of private medical practice they wish, without completing postgraduate training in a specialty. At one time most physicians did not specialize after their internship and established general practices (GP). Today 90% of medical and osteopathic physicians complete a specialty residency and general practice itself is a specialty.
Prior to about 1950 physicians who did not wish to be a GP would list their practice as “limited”. For example, “oculists” were physicians limiting their practice to the eye while others limited their practice to specific organ(s) or diseases. These physicians had not served specialty residencies but had usually stressed those areas while an intern.
After WWII large numbers of young M D.s who served in the armed forces, upon returning home took advantage of the new G.I. Bill to pursue a specialty residency (or attend medical school) and more hospitals began to be built and the country M.D. who once did surgery in the office (or patient’s home) were becoming the minority. Meanwhile early medical insurance plans were forming around larger cities and industrial concerns.
The first specialty to establish board certification after residency was ophthalmology in 1930 to distinguish its practitioners from G.P.s, oculists, EENT doctors, optometrists, opticians and “doctors” who at that time sold mail-order patent medicines that “dissolved cataracts” or “treated” eye weakness.
But until about 1980 the majority of physicians operated private, independent practices, while holding hospital privileges to admit patients for more complex conditions or procedures. In those times the primary purpose of specialty board certification was to signal to their colleagues their area of expertise to enable referrals.
Board Certifications Comes of Age
With the advent of vertical integrations of medical care, public media advertising of health care as a commodity delivered by “providers”, insurance panels, and patients being thought of as “customers” to which TV ads pitched cures, health care changed dramatically and became a fungible business commodity. Its delivery was concentrating around hospitals, HMOs and large group practices and new physicians were becoming employees of them. Growing numbers of specialty procedures became performed only at hospitals or large group practices. The public and insurers became malpractice sensitive, particularly hospitals which used credentialing and privileging for quality control.
Physicians who once had no difficulty in obtaining hospital privileges without being board certified are now often unable to receive privileges. The new specialty of “hospitalist” developed for physicians practicing only within a hospital have no private office but coordinate the care by other specialists within hospitals.
The prime drivers of board certification have become hospitals for quality control purposes while the general public is only vaguely aware of its meaning.
Impact on Optometrists
While board certification is almost mandatory for medical physicians, it is of lesser importance to dentists and optometrists in general practice for which state licensure is the main requirement and hospital privileges not needed.
Podiatrists are affected to the extent they increasingly need to admit patients to hospitals for surgical treatment of below-the-knee conditions and diagnostic scans and tests and have moved, beginning in the 1970s, towards requiring residency training for state licensure. Many of their residency programs also began within VA medical centers and clinics and their utilization within the VA medical system was expanded by the same legislative initiatives applied to optometry in 1976 and equally successful in improving VA care.
Dentists have continued to perform most of their surgical procedures within their private or group offices but have established specialties and board certification programs. Most dentists are in general practice however, have not served residencies and are not board certified in general dentistry.
The majority of optometrists, like dentists, remain in private general practice without need to admit patients to a hospital. The specialty of medical optometry is predominately practiced within accredited medical facilities, optometry-ophthalmology eye centers, group optometry practices and rural optometry practices.
General References
To Err is Human: Building a Safer Health System. Institute of Medicine, National Academy Press. Washington, D.C. ISBN 0-309-06837-1.
The Doctors Mayo, Garden City Publishing Co., Inc. Copyright 1941 by the University of Minnesota.
History of the American Academy of Optometry, James R Gregg. 1987.
Organizational Issues in Health Care Management, Alan Shelton. Spectrum Publications, Inc. 1975.
History of the VA Department of Medicine and Surgery. VA Central Office Library, Washington, D.C.
Bulletin from the Commission On Optometric Specialties, #106, May 29, 1986. AOA St. Louis Office.
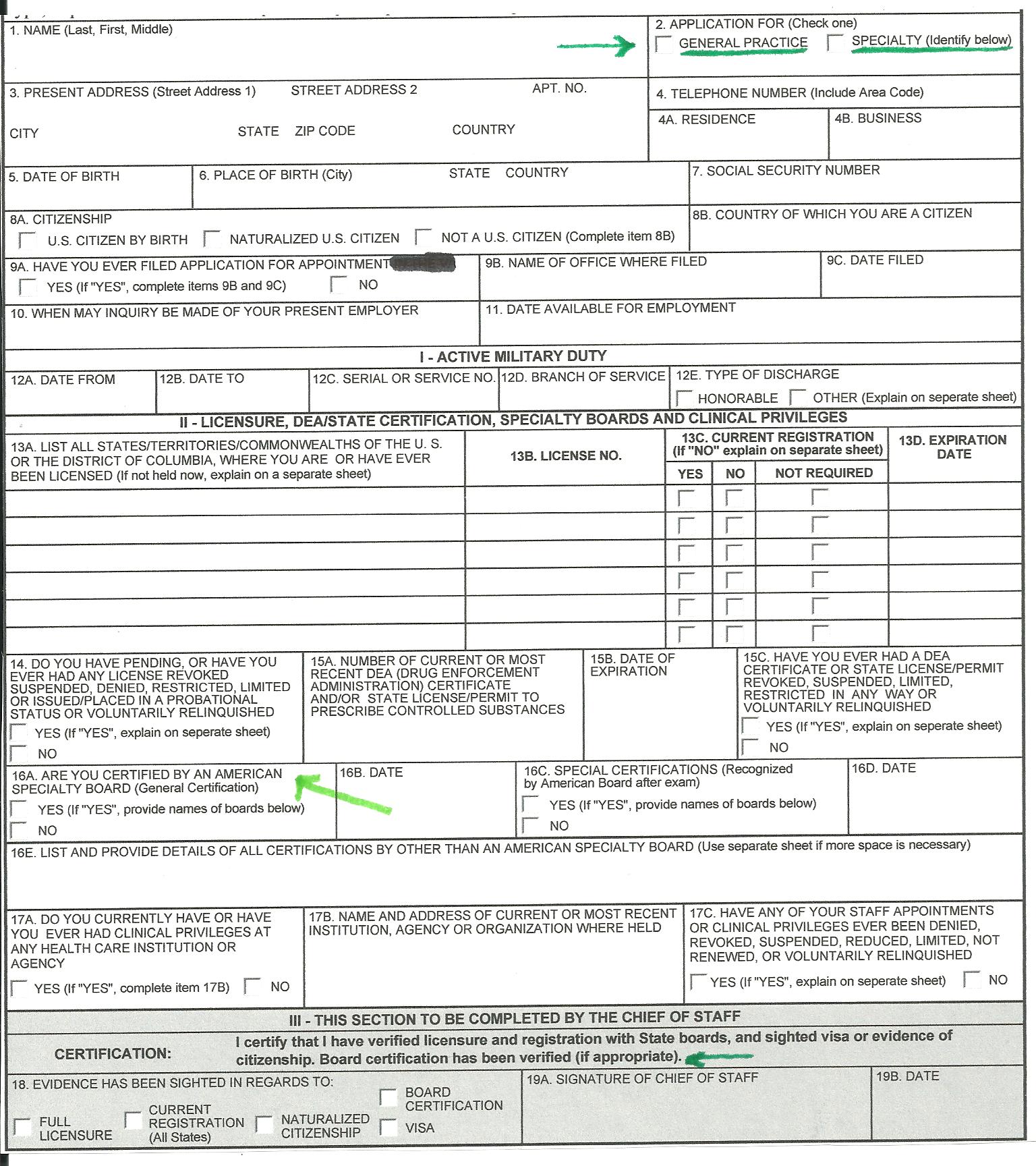
Sample Application Form for “Medicare Physicians”